|
hc8meifmdc|20005939267D|healthm_live|health_library|health_library_details|0xfdff75bd010000004001000001000d00
| For Health Librtary |
| Overview |
|
CoQ10 (coenzyme Q-10) is a vitamin-like naturally occurring compound normally present in every cell of the body. It has a vitamin K like molecular structure and could be considered a relative of vitamin E. It is usually ingested through foods (especially fish and meats) and produced by our bodies, although many people are unable to make Coenzyme Q10 well due to the highly complicated biochemical process required for its production.
CoQ10 is sometimes also referred to as ubiquinol, a name formed with the word ubiquitous (which means "being or seeming to be everywhere at the same time; omnipresent"), because coenzyme Q10 is found in virtually every cell in the body, and with the word quinol coming from the type of coenzyme involved (quinone). All of us have Coenzyme Q10, a coenzyme in our cells called mitochondria. The CoQ10 benefits are derived from its key role by helping the cells to convert fats and sugar into energy called ATP that can be used by our body and various organs like heart and kidney.
By facilitating heart function, Coenzyme Q10 also controls the blood pressure in our body. Our metabolism is impacted greatly by coenzyme levels in the body. Not just for the heart, but also for many organs and muscles, optimum level of coenzyme is essential for overall fitness and health. Since one of the chief CoQ10 benefits is to boost cell metabolism, we call CoQ10, the Super star of mitochondria (cellular) metabolism.
|
| |
| What is CoQ10? |
 |
2-[(2E,6E,10E,14E,18E,22E,26E,30E,34E)-3,7,11,15,19,23,27,31,35,39-decamethyltetraconta- 2,6,10,14,18,22,26,30,34,38-decaenyl]-5, 6-dimethoxy-3-methylcyclohexa-2,5-diene-1,4-dione
Co-enzyme Q10 is a vital antioxidant which is said to produce energy in cells, protects tissues - such as the heart and other vital organs - from free radical damage. |
| |
| Why Ubiquinol is superior to Ubiquinone |
|
Ubiquinone is the oxidized form of CoQ10 and is the more common form of commercially available CoQ10. It has been around for ages, and if you've ever bought one of the cheaper CoQ10 supplements, it has most likely been in the oxidized form. If the label doesn't specifically mention which form of CoQ10 the product contains, it's very probably ubiquinone.
Ubiquinone and Ubiquinol exist together in the body; the body converts ubiquinone into Ubiquinol. CoQ10 as ubiquinone is the "old" form of CoQ10 (by "old" we mean the form that has been commercially available for a long time). The Ubiquinol form is "new" in the commercial sense, and the form touted as being much more absorbable. Coenzyme Q10 exists in both Ubiquinol and ubiquinone forms, but they have vastly different roles to play in the body. For instance, Ubiquinol is an electron donor, while ubiquinone is an electron acceptor. The electrons that Ubiquinol donates neutralize free radicals. This fact alone makes Ubiquinol the form of CoQ10 that protects against toxic oxidative reactions in the body.
The chemical difference between ubiquinone and Ubiquinol is that the Ubiquinol compound contains two hydroxyl groups. These two hydroxyl groups enable Ubiquinol to be more "hydrophilic" than ubiquinone, and thus much easier to assimilate.
The term "hydrophilic" means readily absorbable or dissolvable in water. The two hydroxyl groups on the Ubiquinol compound result in its stronger bonding with water, which helps explain why it is so much more bioavailable than ubiquinone. Ubiquinol has far greater water solubility and much better absorption into the bloodstream after ingestion.
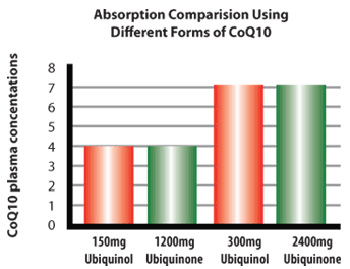
Ubiquinone is the fully oxidized generally sold commercially. Once ingested and absorbed in the body - more than 90% of the ingested Ubiquinone is converted into its "active" antioxidant form called Ubiquinol. More than 90% of the circulating CoQ10 in our body is present as Ubiquinol. The body has reductase enzymes which take the ingested CoQ10 in food and supplements and convert most of it into Ubiquinol. Research, (in animals and humans), has shown Ubiquinol to be absorbed better than Ubiquinone. Therefore, Ubiquinol afford an advantage over ubiquinone.
Ubiquinol, the pre-converted, active antioxidant form of CoQ10, offers the same important health benefits as CoQ10. Because it is pre-converted, Ubiquinol Q10 is ready for immediate use in those 40 and older, and those who have conditions associated with normal aging. This form of CoQ10 is the antioxidant form which neutralizes free radicals and decreases cellular damage. Ubiquinone does not have this antioxidant effect. Since the body converts ubiquinone into Ubiquinol, there is an extra step involved, and not all of the ingested ubiquinone gets converted into Ubiquinol. In healthy people, over 90% of the CoQ10 in the blood is in the form of Ubiquinol, but as you get older, both the total level of coenzyme Q10 and the body's ability to turn it into Ubiquinol decline. This doesn't mean that taking ubiquinone is ineffective; all it means is that taking ubiquinol is more effective. If you are in your twenties or thirties, your body can probably convert much of the ubiquinone into Ubiquinol, If, on the other hand, you are over forty or concerned about your heart health, it may be worthwhile to go for the Ubiquinol. Ubiquinol is already in its reduced form as a potent anti-oxidant. Ubiquinol inhibits protein and lipid oxidation in cell membranes, and helps to minimize oxidative injury to DNA.
Ubiquinol is up to eight times as effective as ubiquinone in increasing blood levels of Ubiquinol. So to get the same effect, you could take one eighth of the amount as Ubiquinol compared to ubiquinone.
Ubiquinol works better for congestive heart failure than Coenzyme Q10. One human study actually does show this claim to be true. (http://www.ncbi.nlm.nih.gov/pubmed/19096107)
Here is a recent case study received by Kaneka, the manufacturer of natural pharmaceutical grade Ubiquinol and ubiquinone:
A 65-year old gentleman with advanced ischemic cardiomyopathy was on maximal medical therapy. In June of 2006, he had low heart function and was receiving 450mg of a soybean oil-based CoQ10 that revealed a level that was sub-therapeutic. He was then given the Ubiquinol formulation at exactly the same dosage of 450mg per day. Three months later, in September of 2006, his CoQ10 level had increased dramatically. Further tests one month later showed a dramatic improvement in heart function and he no longer required any diuretics. By January of 2007, his improvement was great enough that he became quite active and required no further hospitalizations. The case study ended with the physician stating: "This single case represents very striking improvement that I have not seen before in 25 years of cardiology practice...We have now repeated and are continuing to treat several other patients with end-stage or far advanced congestive heart failure with similar remarkable findings."
This study demonstrates the importance of using Ubiquinol, especially as we age. Also, as demonstrated, Ubiquinol does not require the high amount needed by ubiquinone to gain the same therapeutic effect for certain conditions. |
 |
|
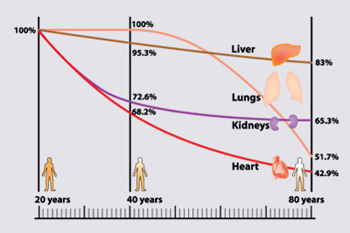 
CoQ10 Level decreases as age increases Effect of Ubiquinol compared to conventional CoQ10(Ubiquinone) |
| |
| How is it Made? |
|
CoQ10 is produced via the fermentation process using a 100% natural yeast food source. All CoQ10 is obtained either by 100% fermentation using a special strain of yeast which yields natural - 100% ALL TRANS CoQ10 - the cheaper synthetic alternative which involves partial fermentation and then synthesis using "solanesol" a chemical extracted from the tobacco leaf. |
| |
| Where is it Found? |
|
Coenzyme Q10 is primarily found in fish and meat. Our bodies are able to produce some of the CoQ10 that we need. The rest is synthesized from the foods we eat. The highest dietary sources of Coenzyme Q10 come from - in descending order according to content - fresh sardines and mackerel, the heart, liver and meat of beef, lamb and pork along with eggs. There are plenty of vegetable sources of Coenzyme Q10, the richest being spinach, broccoli, peanuts, wheat germ and whole grains - in that order, although the amount is significantly smaller than that found in meats. Also, it is important to note that these foods must be raw, fresh and unprocessed - no milling, canning, preserving, freezing, etc., plus grown/produced in an unpolluted environment to be considered viable sources. Oil family is rich in coenzymes Q10. Rapeseed Oil, olive oil, soybean Oil can contribute significant amount of coenzyme. If you are a vegetarian, chances it will be low, so include the coenzyme blood. |
| |
|
|
|
| Benefits / Uses |
|
CoQ10 supplement are considered as a heart strengthener, an energy promoter and an aging fighter and remember that a CoQ10 supplement is just as vital to our bodies as vitamins C and E.
Coenzyme level peaks at teen years. As we age, our coenzyme level and so the CoQ10 benefits gradually reduces. By the time we are 50 years we could have lost half of what we had when we were teens. When we reach 70 years of age, coenzymes in heart wall muscle, pancreas and skin is reduced by 70%. Coenzyme Q10 works exactly like the hormones- they reduce with age. So one of the key anti-aging approaches is to monitor and maintain coenzyme levels so ensure long-term CoQ10 benefits in our body. Since we gain only a very little from natural sources due to conversion (bio availability) issues especially as we get older supplementing to maximize CoQ10 benefits make sense. |
| |
| Congestive Heart Failure Patients |
|
Patients with congestive heart failure have a weak heart. It means the heart works inadequately and the blood volume pumped is very poor. Symptoms of congestive heart failure includes patients having difficulty breathing when lying flat, shortness of breath, accumulation of fluid in lungs, and swelling in lower leg area. Major causes of congestive heart failure include myocardial infarction, cardiomyopathy, and hypertension. Typically myocardial infarction (also know as heart attack) happens after the blockage of a coronary artery, causing cells in the affected area of heart muscle wall to die from lack of blood flow. Due to the heart health CoQ10 benefits, coenzyme supplementation can help patients who suffer from myocardial infarction. |
| |
| Patients Who Take Statin Drugs |
|
Patients who take prescription statin drugs to reduce their cholesterol level will have possible side-effects of statin drug of reduction their coenzyme levels. A Columbia University study in New York found that 30 days of statin therapy (80 mg/day) decreased coenzyme q10 levels by half. Another study by researchers at Kanazawa University in Japan found that smaller doses of statin drugs can reduce Coq10. After eight weeks of 10 mg a day statin therapy, coenzyme q10 levels decreased by 40 percent. Reduced coenzyme Q10 coenzyme levels may result in heart wall as well as other muscle damages. In such cases patients can get coenzymes benefits by taking supplements. There are several studies that have proved that external CoQ10 benefits to counter statin side-effects. |
| |
| Blood Pressure |
|
A randomized, double-blind, placebo-controlled clinical trial of Coenzyme Q10 in Isolated Systolic Hypertension was recently conducted at the Department of Veterans Affairs Medical Center in Boise, Idaho. The conclusion reached at the end of this twelve week study was that CoQ10 may be safely offered to hypertensive patients as a treatment option. The CoQ10 used in this study.
85 patients were enrolled in the study and 80 completed the full 12 weeks (44 men and 36 women). Blood pressures were monitored twice a week between 8:00 AM and 11:00 AM by the same nurse. The project was reviewed and approved by the Institutional Review Board of St. Luke's Regional Medical Center, Boise, Idaho. In the study, patients were randomized to receive twice daily administration of 60mg Coenzyme Q10 soft gels which also contain 150 IU of Vitamin E. The placebo group received a similar appearing soft gel containing Vitamin E alone. |
| |
|
RESULTS: The average reduction in systolic blood pressure (SBP) in the CoQ10 treated group was 18. (Before SBP was 165.1 AFTER SBP was 147.3) In the Placebo group the numbers were: Before SBP was 164.4 AFTER SBP was 162.7). Treatment with the CoQ10 was well tolerated and side-effect rates were comparable to those in the placebo group. The CoQ10 achieved a reduction in blood pressure in 55% of patients which is less than some prescription drugs. However, Coenzyme Q10 is well tolerated and has a high therapeutic index. The lack of any antihypertensive response in 45% of the study participants suggests the possibility of a threshold mechanism of action. Study participants seemed either to respond well or not at all. |
| |
| Parkinson's disease |
|
People with Parkinson's disease could have lower levels of coenzyme Q10. There are some preliminary researches that suggest that CoQ10 supplementation can help increase levels of the neurotransmitter dopamine, which are deficient in people with Parkinson's disease. But the research is inconclusive. There are conflicting information on the strength and the dosage required for treating Parkinson's disease with CoQ10 Benefits. Very high dosage, up to 2000 mg per day may be required to treat Parkinson patients but the results are not typical. |
| |
| Anti Aging, Energy and Fatigue |
|
CoQ10 is an antioxidant and is being sold/used as a dietary supplement. There are benefits to taking a maintenance dose of 50 to 100 mg a day to keep the heart healthy as well as for energy boost. However before one starts a supplement regime, a doctor must be consulted to investigate one's CoQ10 level. Generally if you are below 40 years, you may not need coenzyme Q10. Due to absorption issues, the general rule is that the higher the dose orally administered the lower the percent of the dose absorbed. |
| |
| Summarizing Coenzyme CoQ10 benefits |
 |
Regulates Cellular Metabolism. |
|
|
|
Protects from Congestive heart failure. |
|
|
|
Protect and Improve heart health. |
|
|
|
Regulate Blood pressure. |
|
|
|
Prevent mitochondria and Metabolic disorders. |
|
|
|
As a counter to the side effects of Statin drugs. | | |
| |
| Dosage |
|
The recommended CoQ10 dosage for extended periods of time is between 300-1,000 mg/day (or 100-300 mg/day of Ubiquinol). Patients under statins prescription drugs therapy must consult with a qualified health care provider for the recommended CoQ10 supplement dosage. |
| |
| Possible Side-Effects / Precautions / Possible Interactions: |
|
Caution is advised for patients with diabetes or hypoglycemia for whom it is recommended that blood glucose levels be monitored by a professional health care provider on a regular basis. Adjustments in medications that control blood sugar may be necessary. Another potential Co Q10 side-effect is decrease in blood pressure. Consequently, caution is also advised for people with low blood pressure or taking blood pressure medications. |
| |
| Research Studies / References |
Research conducted at the Alfred Hospital in Melbourne, and funded by the National Heart Foundation of Australia, has shown that CoQ10 may be very valuable to those who undergo heart surgery. Investigators found that elderly heart bypass patients given 300 milligrams of CoQ10 (considered a high dose) recovered better and more quickly than those on placebo. The CoQ10 helped the heart muscle to pump more efficiently and to better tolerate stress.
A series of studies conducted in Japan have reached similar conclusions. Additional research points to CoQ10's ability to help reduce complications and further heart problems after a patient has experienced a first heart attack.
Roland Stocker at the Heart Research Institute in Sydney has come up with data that is relevant to the interests of neurologists. His team has shown that CoQ10 has the ability to target a nasty substance involved in oxidation known as "peroxynitrite." What's important for consideration here is that this substance is, for example, implicated in chronic inflammation, which is a hot topic in research on Alzheimer's disease and other neurodegenerative disorders.
Researchers have demonstrated that Coenzyme Q 10 deficiencies are more prevalent with age. As we grow older, we are no longer able to produce Co Q10 from the food in our diet. This is because as we age, the body loses its efficiency in manufacturing important nutrients. Hence, even though the young may be able to get enough CoQ-10 by making it and ingesting it through diet, a gradual deficiency may develop as we reach middle age and beyond. In addition, people with serious diseases (such as heart disease and cancer) tend to have low Co Q10 levels. Consumed regularly, Coenzyme Q 10 fights off the aging process as it contributes to greater health and longevity.
Many doctors in Europe recommend Coenzyme Q10 supplement to patients with cardiovascular disease (CVD). In Japan, since the late 1970s, Co Q10 supplement has been widely accepted as a preventative dietary supplement and as a treatment for those with heart-related conditions. Since 1982, CoQ10 supplement has rivaled that country's top five medications in consumption. For years, the Japanese have led the world in research on this amazing nutrient.
|
| |
| Potential indications for testing CoQ10 deficiency |
|
Mitochondrial disease. |
|
|
|
Cardiomyopathy. |
|
|
|
Muscular Dystrophy, Parkinson's disease. |
|
|
|
Metabolic syndrome, Malnutrition. |
|
|
|
Patients with coronary artery disease being treated with Statin drugs. |
|
|
|
In the mid 1970's, the Japanese perfected the industrial technology of fermentation to produce pure CoQ10 in significant quantities. To this day, virtually all CoQ10 still comes from Japan. There are two different methods of manufacture. One is via fermentation and the other is via a combination of fermentation and synthesis. |
|
|
|
In the early 1970s, there were discoveries that people with gum disease and heart disease were deficient in CoQ-10. The momentum began to build and, by the early 1980's, CoQ-10 had reached a level of consumption in Japan that rivaled that country's five top medications. In fact, all along, it has been the Japanese and the Europeans who have conducted the majority of clinical trials using CoQ-10 | | |
| |
| References |
| (Cardiovascular Disease) |
|
R.Aejmelaeus, T.Mets,,-Ketel,,, P.Laippala, H.Alho, T.Solakvi. Ubiquinol-10 and total peroxyl radical trapping capacity of LDL lipoproteins during aging: the effects of Q-10 supplementation. Molecular Aspects of Medicine, 1997; 18:Suppl:s113-20. |
|
|
|
R.Alleva, M.Tomasetti, S.Bompadre, G.P.Littarru. Oxidation of LDL and their subfractions: kinetic aspects and CoQ10 content. Molecular Aspects of Medicine, 1997;18:Suppl:s105-12. |
|
|
|
E.Baggio, R.Gandini, A.C.Plancher, M.Passeri, G.Carmosino. Italian multicenter study on the safety and efficacy of coenzyme Q10 as adjunctive therapy in heart failure. CoQ10 Drug Surveillance Investigators. Molecular Aspects of Medicine 1994;15 Suppl:s287-94. |
|
|
|
A.M.Bargossi, M.Battino, A.Gaddi, P.L.Fiorella, G.Grossi, G.Barozzi, R.Di Giulio, G.Descovich, S.Sassi, M.L.Genova. Exogenous CoQ10 preserves plasma ubiquinone levels in patients treated with 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors. Int J Clin Lab Res 1994;24(3):171-6. |
|
|
|
R.F.Beyer, L.Ernster. The antioxidant role of coenzyme Q. Highlights in Ubiquinone research. G.Lenaz, O.Barnabei, A.Rabbi, M.Battino, (Eds) Taylor and Francis, London, 1990, pp.191-213 |
|
|
|
M.Chello, P.Mastroroberto, R.Romano, E.Bevacqua, D.Pantaleo, R.Ascione, A.R.Marchese, N.Spampinato. Protection by coenzyme Q10 from myocardial reperfusion injury during coronary artery bypass grafting. Ann Thorac Surg 1994 Nov;58(5):1427-32. |
|
|
|
M.Chello, P.Mastroroberto, R.Romano, P.Castaldo, E.Bevacqua, A.R.Marchese. Protection by coenzyme Q10 of tissue reperfusion injury during abdominal aortic cross-clamping. J Cardiovasc Surg (Torino) 1996 Jun;37(3):229-35. |
|
|
|
Y.F.Chen, Y.T.Lin, S.C.Wu. Effectiveness of coenzyme Q10 on myocardial preservation during hypothermic cardioplegic arrest. J Thorac Cardiovasc Surg 1994 Jan;107(1):242-7. |
|
|
|
A.Constantinescu, J.J.Maguire, L.Packer. Interactions between ubiquinones and vitamins in membranes and cells. Molecular Aspects of Medicine, 1994;15 Suppl:s57-s65. |
|
|
|
F.L.Crane, Y.Hatefi, R.I.Lester, C.Widmer. Isolation of a quinone from beef heart mitochondria. Biochimica et Biophys. Acta 1957;25:2201. |
|
|
|
F.L.Crane, D.J.MorrÅ . Evidence for coenzyme Q function in Golgi membranes. In: K.Folkers, Y.Yamamura (Eds) Biomedical and Clinical Aspects of Coenzyme Q. Elsevier, Amsterdam; 1977; p.77-86. |
|
|
|
F.L.Crane, I.L.Sun, R.Barr, D.J.MorrÅ . Coenzyme Q in Golgi apparatus membrane redox activity and proton uptake. K.Folkers, Y.Yamamura (Eds) Biomedical and Clinical Aspects of Coenzyme Q. Elsevier, Amsterdam; 1984;4:77-86. |
|
|
|
J.A.Crestanello, J.Kamelgard, D.M.Lingle, S.A.Mortensen, M.Rhode, G.J.Whitman. Elucidation of a tripartite mechanism underlying the improvement in cardiac tolerance to ischemia by coenzyme Q10 pretreatment. J Thorac Cardiovasc Surg, 1996 Feb;111(2) 443-50. |
|
|
|
V.Digiesi, F.Cantini, A.Oradei, G.Bisi, G.C.Guarino, A.Brocchi, F.Bellandi, M.Mancini, G.P.Littarru. Coenzyme Q10 in essential hypertension. Molecular Aspects of Medicine, 1994;15 Suppl:s257-63. |
|
|
|
L.Ernster, P.Forsmark-Andree. Ubiquinol: an endogenous antioxidant in aerobic organisms. K.Folkers, S.A.Mortensen, G.P.Littarru, T.Yamagami, and G.Lenaz (eds) The Clinical Investigator, 1993;71(8):S60-5. |
|
|
|
K.Folkers, G.P.Littarru, L.Ho, T.M.Runge, S.Havanonda, D.Cooley. Evidence for a deficiency of coenzyme Q10 in human heart disease. Int Z Vitaminforsch, 1970; 40(3):380-90. |
|
|
|
K.Folkers, S.Vadhanavikit, S.A.Mortensen. Biochemical rationale and myocardial tissue data on the effective therapy of cardiomyopathy with coenzyme Q10 . Proc Natl Acad Sci U S A, 1985 Feb; 82:3, 901-4. |
|
|
|
K.Folkers, P.H.Langsjoen, R.Willis, P.Richardson, L.J.Xia, C.Q.Ye, H.Tamagawa. Lovastatin decreases coenzyme Q levels in humans. Proc Natl Acad Sci U S A, 87: 22, 1990 Nov, 8931-4. |
|
|
|
G.Ghirlanda, A.Oradei, A.Manto, S.Lippa, L.Uccioli, S.Caputo, A.V.Greco, G.P.Littarru. Evidence of plasma CoQ10 -lowering effect by HMG-CoA reductase inhibitors: a double-blind, placebo-controlled study. J Clin Pharmacol 1993 Mar;33(3):226-9. |
|
|
|
M.Hamada, Y.Kazatani, T.Ochi, T.Ito, T.Kokubu. Correlation between serum CoQ10 level and myocardial contractility in hypertensive patients. Biomedical and Clinical Aspects of Coenzyme Q, Elsevier, Amsterdam 1984;4:263-70. |
|
|
|
K.Hashiba, K.Kuramoto, Z.Ishimi, K.Kato, K.Seki, K.Taniguchi, T.Taya, F.Terawasa, S.Torii, J.Fijii, N.Yamazaki and H.Watanabe, Heart 1972;4:1579-89 [in Japanese]. |
|
|
|
Y.Hiasa, T.Ishida, T.Maeda, K.Iwanc, T.Aihara, and H.Mori. Effects of coenzyme Q10 on exercise tolerance in patients with stable angina pectoris. K.Folkers, Y.Yamamura (eds) Biomedical and Clinical Aspects of Coenzyme Q. Elsevier, Amsterdam; 1984;4:291-301. |
|
|
|
K.U.Ingold, V.W.Bowry, R.Stocker, C.Walling. Autoxidation of lipids and antioxidation by alpha-tocopherol and ubiquinol in homogeneous solution and in aqueous dispersions of lipids: unrecognized consequences of lipid particle size as exemplified by oxidation of human low density lipoprotein. Proc Natl Acad Sci U S A 1993 Jan 1;90(1):45-9. |
|
|
|
T.Iwabuchi, N.Kato, N.Goto, Y.Higuchi, S.Takaola, Y.Iwaki, E.Shidara, M.Yoshimura and J.Atarashi. Jpn. J Clin. Exp. Med. 1972;49:2604-8 (in Japanese). |
|
|
|
W.V.Judy, J.H.Hall, P.D.Toth, K.Folkers. Double blind-double crossover study of coenzyme Q10 in heart failure. In: K.Folkers and Y.Yamamura (eds) Biomedical and Clinical Aspects of Coenzyme Q, Elsevier, Amsterdam; 1986;5:315-23. |
|
|
|
W.V.Judy, K.Folkers, J.H.Hall. Improved long-term survival in coenzyme Q10 treated congestive heart failure patients compared to conventionally treated patients. K.Folkers, G.P.Littarru and T.Yamagami (eds) Biomedical and Clinical Aspects of Coenzyme Q. Elsevier, Amsterdam; 1991;6:291-8. |
|
|
|
W.V.Judy, W.W.Stogsdill, K.Folkers. Myocardial preservation by therapy with coenzyme Q10 during heart surgery. Clinical Investigator 1993;71(8 Suppl):S155-61. |
|
|
|
T.Kamikawa, A.Kobayashi, T.Yamashita, H.Hayashi, and N.Yamazaki. Effects of coenzyme Q10 on exercise tolerance in chronic stable angina pectoris. American. Journal of Cardiology 1985; 56:247-51. |
|
|
|
T.Kato, S.Yoneda, T.Kako, M.Koketsu, I.Hayano, T.Fujinami. Reduction in blood viscosity by treatment with coenzyme Q10 in patients with ischemic heart disease. Int J Clin Pharmacol Ther Toxicol 1990 Mar; 28 (3):123-6. |
|
|
|
T.Kishi, T.Okamoto, N.Kanamori, T.Yamagami, H.Kishi, A.Onada and K.Folkers. Estimation od plasma levels of coenzyme Q10 and relationship to oral dosage. K.Folkers, Y.Yamamura (eds) Biomedical and Clinical Aspects of Coenzyme Q. Elsevier/North-Holland Press;1981;3:67-89. |
|
|
|
N.Kitamura, A.Yamaguchi, M.Otaki, O.Sawatani, T.Minoji, H.Tamura, and M.Atobe. Myocardial tissue level of coenzyme Q10 in patients with cardiac failure. K.Folkers and Y.Yamamura (eds) Biomedical and Clinical Aspects of Coenzyme Q. Elsevier, Amsterdam; 1984;4:243-52. |
|
|
|
B.Kuklinski, E.Weissenbacher, A.Fahnrich. Coenzyme Q10 and antioxidants in acute myocardial infarction. Molecular Aspects of Medicine, 1994;15 Suppl:s143-7. |
|
|
|
R.Laaksonen, K.Jokelainen, T.Sahi, M.J.Tikkanen, J.J.Himberg. Decreases in serum ubiquinone concentrations do not result in reduced levels in muscle tissue during short-term simvastatin treatment in humans. Clin Pharmacol Ther 1995 Jan;57(1):62-6. |
|
|
|
P.H.Langsjoen, S.Vadhanavikit, K.Folkers. Response of patients in classes III and IV of cardiomyopathy to therapy in a blind and crossover trial with coenzyme Q10 . Proceedings of the National Acadademy of Sciences, U.S.A. 1985; 82:4240-4. |
|
|
|
P.H.Langsjoen, P.H.Langsjoen, K.Folkers. Long-term efficacy and safety of coenzyme Q10 therapy for idiopathic dilated cardiomyopathy. American. Journal of Cardiology, 1990, Feb 15; 65(7):521-3. |
|
|
|
P.H.Langsjoen, P.H.Langsjoen, K.Folkers. Isolated diastolic dysfunction of the myocardium and its response to CoQ10 treatment. K.Folkers, S.A.Mortensen, G.P.Littarru, T.Yamagami, and G.Lenaz (eds) Clinical Investigator,1993;71:S140-4. |
|
|
|
H.A.Langsjoen, P.H.Langsjoen, P.H.Langsjoen, R.Willis, K.Folkers. Usefulness of coenzyme Q10 in clinical cardiology: a long-term study.Molecular Aspects of Medicine, 1994;15 Suppl:s165-75. |
|
|
|
P.H.Langsjoen, P.H.Langsjoen, R.Willis, K.Folkers. Treatment of essential hypertension with coenzyme Q10 . The Molecular Aspects of Medicine, 1994;15 Suppl:s265-72. |
|
|
|
P.H.Langsjoen, A.Langsjoen, R.Willis, K.Folkers. Treatment of Hypertrophic Cardiomyopathy with Coenzyme Q10 . Molecular Aspects of Medicine, 1997;18 Suppl.:s145-51. |
|
|
|
P.H.Langsjoen, A.Langsjoen, R.Willis, K.Folkers. The Aging Heart: Reversal of Diastolic Dysfunction Through the Use of Oral CoQ10 in the Elderly. Anti-Aging Medical Therapeutics, 1997b, R.M.Klatz and R.Goldman (eds), Health Quest Publications, pp.113-120. |
|
|
|
A.Lawen, R.D.Martinius, G.McMullen, P.Nagley, F.Vaillant, E.J.Wolvetang, A.W.Linnane. The universality of bioenergetic disease: The role of mitochondrial mutation and the putative inter-relationship between mitochondria and plasma membrane NADH oxidoreductase. Molecular Aspects of Medicine, 1994;15: s13-s27. |
|
|
|
G.Lenaz and G.Parenti Castelli. Biological Membranes G. Benga (ed), CRC Press, Boca Raton, USA 1984 Vol. I. |
|
|
|
G.Lenaz and D.Esposti. Physical properties of ubiquinones in model systems and membranes. In: G.Lenaz (ed). Coenzyme Q. Biochemistry, Bioenergetics and Clinical Applications of Ubiquinone. John Wiley & Sons; 1985; Chapter IV, p.83-105. |
|
|
|
G.Lenaz. The role of mobility of redox components in the inner mitochondrial membrane. J. Membr. Biol. 1988;104:193-209. | |
| | |
|